And the Dance Goes On: Psychological Impact of Injury
Lynda M. Mainwaring, Ph.D., C.Psych., Donna Krasnow, M.S., and Gretchen Kerr, Ph.D.
Journal of Dance Medicine & Science, Volume 5, Number 4, 2001.
Abstract
This review provides a glimpse into the dancer’s psychological reaction to physical injury. Based on the current evidence, dancers’ reactions to injury involve initial negative affects that may become more positive as the injury heals. Dancers with chronic or overuse injuries are more likely to ignore the injury, sometimes to the point of more severe damage and psychological distress. There is evidence that the impact of injury may vary across different types of injury (acute, chronic, overuse, recurrent), individual differences in personality, levels of knowledge and available information about injury and recovery, and styles of coping and social support. Dancers continue to dance with injury, pain and discomfort, perhaps to avoid the “disruption of self ” that emanates from injury, and perhaps because of the embedded subculture in dance that embraces injury, pain, and tolerance. Some implications of these findings for future research, teaching, and clinical practice are discussed.
Since approximately 1975, information on the nature, incidence, prevalence, and risk factors of dance injuries has multiplied.[1] Even though dance is not a high-risk activity, research shows that most dancers have experienced injury during their careers.[2-5] Different dance forms seem to promote different patterns of injury. For example, injuries to the foot, ankle, knee, and back are common in ballet,[1,5-7,9] knee and back injuries are more frequently reported by modern dancers,[1,6,8,10] and sesamoiditis is common in flamenco.[11] Whatever the dance form, there is risk of injury, depending on extrinsic factors (e.g., training environment, floor surface, shoe condition, and performance and rehearsal schedule) and intrinsic factors (e.g., age, personality, fatigue, psychological stress, and social support). Dance medicine, and the budding field of dance psychology, have only recently begun to address the psychological precursors and sequelae of injuries in dance. A few empirical studies have examined psychological factors that may be associated with injury occurrence;[7,12,13] however, very little research exists regarding the psychological impact of injury on the dancer. Despite this current gap, it is evident from existing studies,[4,13-16] clinical observation, and anecdotal accounts that physical injury concurrently affects a dancer’s psychological and social health and well-being.
Only in the last few years has dance psychology emerged as an area of scholarly activity. It follows the lead of sport psychology, yet has distinct issues for examination. Dancers face unique challenges in terms of the injury and rehabilitation experiences. To begin with, dancers are reluctant to acknowledge being injured for fear of being replaced in a performance and losing potential income. There is pressure from choreographers, peers, and the dancers themselves to continue to rehearse and perform despite pain and injury, simply because the show must go on. When dancers do seek treatment for their injuries they tend to pursue nontraditional modalities. They too often feel misunderstood and inadequately treated by medical professionals, who they believe lack an appreciation of the dance world. Thus, dancers have quite different values and priorities from people in mainstream careers. In what other profession does one train for 10 years or more, investing time, money and energy, with the knowledge that gainful employment is uncertain and that even success may involve living at poverty levels?
Recently researchers have begun to investigate these matters. This special issue of this journal is evidence of the topic’s importance, and the dance medicine and science community’s commitment to understanding and advancing matters germane to the psyche of dancers in relation to injury prevention, education, and treatment. This study will provide an overview of the current state of knowledge regarding the psychological and psychosocial impact of injury on the dancer. Existing scientific information is reviewed, followed by an overview of implications for research and practice.
Psychological Reactions to Athletic Injury
We can look to sport psychology to begin to understand the psychological consequences of injury for the dancer. In the 1980s investigators began to explore athletes’ reactions to injury and rehabilitation.[17-21] They started by examining the postulate that the reaction to sport injury is the same as the grief reaction associated with death and dying. Elizabeth Kubler-Ross’ five-stage theory (shock/denial, anger, bargaining, depression, and acceptance) was presumed to describe an athlete’s psychological experience following injury. However, this presumption proved not to be supported by empirical evidence; it was based solely on anecdotal evidence and speculation. Over the past 12 years research has flourished concerning the psychology of athletic injury. Numerous studies have investigated the impact of injury,[20-25] and theory development is well underway. [22-26] Evidence strongly suggests that Kubler-Ross’ theory does not explain an athlete’s reaction to physical injury; however, one still may stumble upon written and verbal discussions that endorse a similarity.[27,28]
Empirical studies, both quantitative and qualitative, suggest that there are cognitive, emotional, and social consequences of sport injury. [22,24,29-31] Injured athletes experience a variety of emotions that are initially, and primarily, negative, followed by moments of optimism. [24] Andersen and Williams[22] proposed a stress response model that hypothesizes the following factors as influences on injury occurrence: personality (e.g., competitive trait anxiety, locus of control, hardiness, achievement motivation), history of stressors (previous injuries, life events), and coping resources (social support, coping behaviors). A number of studies have supported their model.[32] Wiese- Bjornstal and colleagues developed an integrated model of response to sport injury that builds on Andersen and Williams’ pre-injury model.[26,22] This model depicts factors hypothesized to influence athletes’ response to injury (person factors such as injury experience, and individual difference factors such as psychological, demographic, and physical factors), as well as features of the actual response (cognitive, emotional, and behavioral). Brewer developed a cognitive appraisal model of psychological adjustment to athletic injury.[23] It suggests that personal and situational factors lead first to a cognitive appraisal of the injury, which in turn leads to an emotional response, and then a behavioral response to injury and rehabilitation. According to Brewer, cognitive appraisal models account for individual differences in response to injury, whereas grief models do not. Consistent with stress and coping models, cognitive appraisal models focus on the cognitive interpretation of injury. Data driven models that describe the experience of injury from the athletes’ perspective have been offered by Rose and Jevne[25] and by Mainwaring.[24] Rose and Jevne proposed four phases in the impact of injury: getting injured, acknowledging the injury, dealing with the impact of the injury, and achieving a physical and social outcome. Mainwaring’s model suggests an interaction between the injured athlete’s experience of injury (the person) and the environment (the situation), and depicts a holistic reaction that is multidimensional rather than linear.[24] It outlines psychological, physical, and social consequences and experiences of injury. All of the models cited are based on empirical and clinical evidence, and none support Kubler-Ross’ grief theory as relevant for injured athletes.
In essence, the current empirical work on the impact of athletic injury reveals that athletes view injury as stressful, and its consequence may disrupt an athlete’s sense of identity. [33] For first-time serious injuries, athletes experience shock, frustration, depression, anxiety, fear, and anger in the first few weeks post injury. [4,24,25,31,34,35] Fluctuations in negative and positive emotion occur in relation to daily events and progress in rehabilitation. Optimism and happiness are often associated with perceived gains in rehabilitation, [24,36,37] whereas the corollary – greater pain, frustration, fear, and pessimism – may be experienced in relation to decreases in range of motion.[37] Athletes seem to cope differently with second-time or third-time injuries than they do with first-time injuries,[38] and differently with chronic and acute injuries. [39] Johnson reported that multiply- injured athletes had greater capacity to accept injury, higher levels of social orientation and activity, and less anxiety about subsequent injuries than did first-time injured athletes.[38] In addition, they experienced injuries as less stressful and threatening. Johnson suggests that experience with severe injury facilitates certain psychological and psychosocial qualities: belief in one’s own inherent capacity to proceed through rehabilitation, the power to cope actively with and master the stressful injury experience, and the ability to maintain contact with friends and family. Smith found that seriously injured athletes had significantly more tension, depression, and anger, and lower vigor, than those with less serious injuries.[40] In general, the emotional reaction to severe athletic injury involves increased depression, anger, frustration, [31,41] shock,[24,27] fear,[24,29,35,37] and lowered self-esteem.[30]
The methodologies used to examine athletes’ reactions to injury have varied in type and quality. Most of the early research involved case studies and retrospective selfreport studies. More recently, strong research designs have provided a clearer understanding. Large-scale prospective control group studies have shown a change in emotional profiles pre-injury and post-injury.[30] For example, Leddy and associates showed that when compared to preinjury measures, injured athletes were more fatigued and depressed, and less vigorous.[30] In addition, there have been prospective studies that examined the injured athlete’s personal struggle, particularly with anterior cruciate ligament injuries. [24,29,37] For the most part, the research on impact of injury in the sport psychology literature has been conducted with methodological rigor, and reveals a general picture of how athletes respond to injury. The details of that picture are being explored through continued inquiry.
The field of sport psychology has also examined the role psychology can play in injury rehabilitation. Numerous suggestions for psychological intervention have emerged from clinical experience,[7,19,21] current empirical research, and studies that specifically examine rehabilitation issues.[42-46,48] In general, the guidelines to facilitate recovery are a blend of sound clinical psychology practice and sport psychology strategies that have been used for performance enhancement (goal setting, relaxation, positive self-talk, and so forth).[49,50]
Psychological Impact of Dance Injury
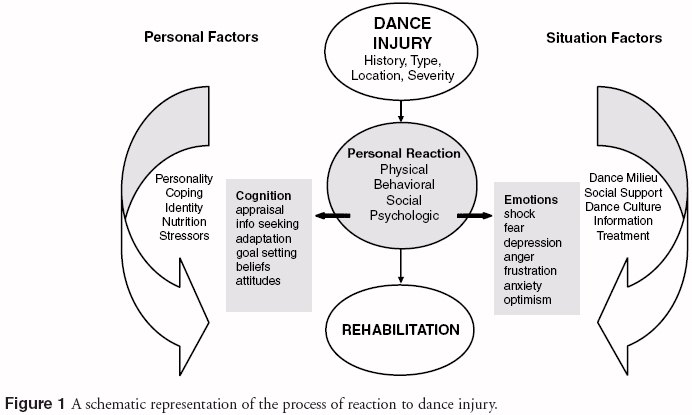
The psychological impact of injury on the dancer involves a number of personal and situational factors. As a point of reference for the following discussion these factors are represented schematically in Figure 1.
Recent research in dance medicine and science provides evidence that a variety of injuries in dance are common, if not inevitable.[1,13,51] Often injuries are ignored by the dancer[52] and frequently not reported to a physician.[53,54] Research that explores psychological and psychosocial sequelae of dance injury may uncover a rationale for such behavior. A high prevalence of dance injuries has been revealed in studies that used self-report, rather than medical diagnosis, to identify injury. One prospective study reported that 38 of the 39 dancers in the subject base (97%) were injured during the course of the investigation, with a mean of 2.4 injuries per dancer.54 Macchi and Crossman found that all 26 of the dancers they interviewed had been injured at least once during their career, with a mean injury rate per dancer of 2.7 (range: 1 to 5 injuries).[4] In a similar age group, Krasnow and coworkers reported that 15 of 16 ballet dancers (94%) and 15 of 19 modern dancers (79%) were injured.[2]
Type and incidence of injuries vary across dance forms and age. Schafle and colleagues reported that of 3,251 dance-related injuries, 55% were seen in ballet, 15% in modern, and 30% in aerobic dancers. The greatest proportion of ballet injuries was found in 13 to 18 year olds. The authors reported that 43% of the ballet injuries occurred in dancers younger than 16 years of age.[55] A closer inspection of the intrinsic factors associated with injuries across genre and age may provide insight into injury patterns and the barriers to reporting and treatment.
We know that the great majority of injuries in dance are overuse injuries, [1,56] which tend to be accompanied by pain and discomfort, a lack of understanding for the injury, and psychological sequelae that typically are unrecognized or ignored. [54] Theatrical dance has evolved a “culture of tolerance” concerning injury and pain that encourages dancers to dance through, around, and in spite of injury. If the physical injury is ignored, the psychological impact of injury clearly has not been, and probably will not be, addressed. With the increased attention to the nature and prevalence of dance injuries, along with the research on psychological aspects of athletic injury emanating from sport psychology, an appreciation for the emotional side of injury has evolved in the dance science community.
Emotional Reaction
The emotional reaction to injuries sustained by dancers has been investigated in three studies to date.[4,7,14] Similar to the findings in sport psychology, dancers’ emotions immediately post-injury are negative and progress to more positive feelings with recovery. Macchi and Crossman examined the impact of injury on 26 professional ballet dancers between the ages of 12 and 21.[4] Retrospective accounts of injuries were collected through semistructured interviews, and revealed that the predominant emotions recalled for the initial period after injury (typically ankle and back sprains) included frustration, fear, distress, anger, and depression. Several dancers indicated that they were initially afraid of the reaction of others (teachers, staff, parents, and other dancers), and what impact the injury would have on their career. Watching class provoked feelings of guilt and anger. During rehabilitation, reactions varied from optimism about resuming their careers to pessimism about the severity of the injury and time needed to recover. Macchi and Crossman’s qualitative study provided information regarding dancers’ recollections of reactions to injuries incurred over their careers. The authors emphasized that one of the main limitations to their research is the bias inherent in retrospective self-reports. Another limitation is the heterogeneity of the type and severity of injuries. Consequently, we cannot discern from this research whether the reactions noted are to mild, moderate, severe, overuse, acute, chronic, or recurrent injuries, nor whether reactions to a severe back strain, for example, are commensurate with those to an ankle sprain.
Mainwaring and Krasnow interviewed two young injured dancers (16 and 18 years of age) whose retrospective accounts of their chronic debilitating hip injuries revealed a preponderance of negative emotions throughout the injury period.[14] For both, there was a mix of anger, uncertainty, jealousy, frustration, anxiety, feelings of alienation, depression, guilt, self-doubt, disappointment, and fear. In these cases the dancers also experienced anger, guilt, and distress about watching others dance. In addition, they continued to perform movements that evoked pain that was recognized as a sign that something was wrong. Both dancers experienced coping difficulties that resulted in psychotraumatic distress, manifested by an attempted suicide in one case and depressive episodes and disordered eating in the other. One of the dancers also went through bouts of self-mutilation, in the form of selfcutting, and used clothing to hide the symptoms. The severity of the negative psychological impact on the lives and experience of these two young aspiring dancers is obvious, but one must be cautious in attributing these traumatic experiences to the injury occurrence alone. The dancers’ recollections and perceptions were made available because of their willingness to share their experiences of injury in an interview; it was not a psychological assessment.
Liederbach and colleagues followed 12 professional ballet dancers (6 female and 6 male, with mean ages of 24 and 26, respectively) for 5 weeks of an intensive season.7 At injury onset they found increased fatigue and inertia, decreased vigor and energy, and increased secretion of urinary catecholamines, a measure of sympathoadrenal activity, and thus stress. The majority of the injuries (75%) were categorized as “overuse injuries.” The authors concluded that:
1. The increase in catecholamine “may be a reaction to performance- related psychological and/or physiological stress,”[7] and
2. Injury trends in their study appeared to be closely tied to time-specific onset of performance- related psychological and physical stress. We cannot determine cause and effect from this study, but it certainly points to some interesting associations between the physical and psychological precursors and reactions to injury. The study of psychophysiological indicators of the stress response associated with injury is an area that sport psychology is pursuing currently, and dance science has embarked upon.
Pain
Pain is an obvious psychosociophysiological reaction to injury. What is familiar to the dancer and clinician is finally gaining the respect of scientific investigation. Tajet-Foxell and Rose found that dancers, like athletes, exhibited higher pain thresholds and tolerance than non-dancers.[57] These investigators suggested that the “mostlikely” explanation is the higher exposure to fitness and training, and thus higher circulating endogenous opioids, for elite performers compared with a control population.[58] However, they cautioned that one should not overlook a possible psychological explanation that attributes higher pain thresholds in dancers and athletes to their familiarity with the interface between physical activity and pain. They suggested that the multidimensional study of pain in dancers and athletes has received insufficient attention, and that studies using threshold measures only may not reveal a complete picture, nor lend themselves to correct interpretation. They concluded that “the meaning of pain, the importance of acknowledging pain and of learning how to respond to it, should be targeted as early as possible in a dancer’s training.”[57]
Ramel and associates reported that older ballet dancers, despite an increase in age and workload, do not report more incapacitating pain than their younger colleagues.59 Similarly, Encarnacion and coworkers found no difference in pain coping styles among groups of 135 ballet dancers of varied skill levels.[60] Again, this research suggests that dancers, regardless of skill or age, are trained to cope with pain and injuries in a particular way. The authors also noted that ballet performers exhibited lower coping and cognitive skills and higher catastrophising responses than recreational runners, high school and collegiate intramural athletes, rodeo performers, and elite equestrians. In short, Encarnacion and coworkers suggested that ballet dancers do not exhibit pain coping styles similar to those of other sport performers. However, it needs to be acknowledged that the assessment of pain and coping styles is not uniform across studies: there are numerous measures of pain and coping. In addition, the study by Encarnacion and coworkers did not account for current injuries, time of season, history of injuries, or type and severity of injury – all issues that have impact on the injury experience and its evaluation. Moreover, the instrument used in this case was the Sports Inventory for Pain (The SIP), which “measures 5 sub-scales relevant to competition” (not aesthetic activity), and may not be a valid measure of pain and coping issues in dance.[61] For example, the authors state that the coping sub-scale “seems to measure the extent to which an athlete utilizes ‘direct’ coping strategies. High scorers tend to ignore pain, realize that pain is part of competition, and in general tend to ‘tough it out.’”[60] Furthermore, this questionnaire does not differentiate between first-time or subsequent injuries, or chronic or acute injuries.
It seems reasonable, given that dancers suffer more overuse injuries than athletes, to postulate that dancers, or those who suffer overuse injuries in general, cope quite differently than those who suffer traumatic injuries. Living day to day with pain and discomfort wears on the body and psyche such that it is likely that different coping styles or strategies are developed (it has been suggested previously that persistent daily hassles are much more detrimental to the body’s immune system than are acute bouts of stress[62]). Consequently, research into pain and coping of dancers needs to address the unique issues and circumstances of dancers. Stating that dancers have lower coping and cognitive skills and higher catastrophising scores than athletes probably promotes an inaccurate idea that dancers do not cope with injuries as well as athletes do. The truth of the matter lies in the assessment of pain and coping in relation to all the important moderator variables (type and severity of injury, history of injury, and so forth), and to what is known of the dance population itself, especially if the personality of a dancer varies from that of an athlete.[63] As an example of this approach, Pedersen and Wilmerding suggested that flamenco dancers are not well apprised of injury prevention and rehabilitation techniques, and consequently continue to dance despite painful injuries.[52] Sesamoiditis is such a common problem for this population, the authors reported, that many dancers do not consider it an injury. Hence, the habit of ignoring pain may simply be a by-product of the dance form.
With the adolescent dance population specifically, there is risk of the following:
1. Young dancers having insufficient knowledge of injuries, anatomy, and the injury-andrecovery process to manage their injuries themselves, and
2. Students hiding pain in their attempt to please or gain the approval of their teachers, and thereby exposing themselves to further damage.[14]
Consequently, research into the pain and coping experiences of dancers across age groups would be useful.
The Role of Person Factors
The role that person factors, such as personality, motivation, identity, and injury history, play in recovery from dance injury has not been well established. Few studies have examined the relationship between personality and injury. Krasnow and colleagues explored the relationships among perfectionism, stress, and injury.[2] They found differences among sub-scales of perfectionism, negative and positive stress, and injury. The authors recommended further research of psychological correlates of the stress-injury phenomenon.
It is clear from the literature on illness and health that a person’s disposition plays a major role in rehabilitation. For example, optimists tend to cope more effectively after surgery[63-69] and after athletic injury. [24] Similarly, hardiness has been found to be negatively associated with total mood disturbance in relation to athletic injury.[45] Observation reveals that dancers exhibit hardiness in relation to overuse injuries in that they often endure pain and discomfort in order to rehearse and perform. The following quotation from two experts in dance medicine and science (one a former dancer) alludes to this personality trait:
To survive and ascend, a dancer must be self-analytical and selfcritical virtually to a fault. For dancers, dance is more than an art; it is an all-consuming lifestyle. The aesthetic, the technique, the teachers, and perhaps most importantly, the dancer must constantly push to exceed, to overcome, to persist and to persevere. The love of dance and desire to dance are intrinsic to dancers of all levels and talent. Many have sacrificed so much just to have those few moments of pure movement where the physical price was no measure of the artistic reward.[68]The image one has of oneself, or identity, is often defined by one’s work. For dancers, their work is their dancing: it is a way of life that defines who the dancer is. Therefore, any barrier to self-expression and movement may be a threat to a dancer’s identity.
Identity is the most examined person factor in recovery from athletic injury.[46] The research suggests that the more narrowly defined the sense of self, the more threatened the athlete will be by any challenge to identity. In the case of injury, the more an athlete’s self-identity is linked to his or her role as athlete, the more likely reactions to injury will be negative (e.g., feelings of anxiety, depression, or hopelessness).[31,33] The fundamental loss of self that accompanies chronic illness or injury[69,70] or athletic injury,[24,71] and the context within which this happens, has been well established in the sport sociology research. [71,72] Moreover, the concept “restoring the self ” after injury is an emergent theme in the psychology and sociology literatures[24,71] that has implications for rehabilitation and treatment. These implications will be discussed in a later section.
Shaffer found that prior experience with successful rehabilitation had a positive impact on assessments of ability to manage subsequent injury.[73] This is consistent with social learning theory and research, which indicates that self-efficacy (the belief that one can accomplish a particular task) is an important mediator of behavior.
Psychosocial Issues
Treatment
A few trends have been identified with respect to the medical and psychosocial issues of injury reporting and treatment. Pedersen and Wilmerding suggested that most foot injuries were not reported to or treated by a physician.[52] Similarly, Kerr and associates found that only 20% of the injuries identified by university dancers were reported to a physician.[54] In the latter study, the dancers indicated that they did not feel comfortable seeing a physician because they perceived that their situations and injuries would not be understood, and that they would be told to stop dancing regardless of the severity of the injury. In general, there was a lack of confidence in medical practitioners.
Ryan and Stephens in their 1988 book wrote that:
until very recently there was little information about the causes, nature and appropriate treatment of dancers’ injuries available to physicians. As a consequence, dancers may have had difficulty in finding physicians who had good understanding of their situation and their particular problems.[68]They indicate that the same was true years ago of athletes and physicians. “Both have learned from cultivating these relationships, and the same thing is possible for dancers.”68 Clearly, the lack of information and understanding about the nature of both the physical and psychosocial impact of dance injuries has affected the treatment available to dancers. Most dancers have not been afforded the luxury of a practitioner who once danced or who specializes in dance injuries. Consequently, the field of dance medicine and science serves a vital educational function in the lives of dancers and those who treat them. As Trepman points out, “the primary goal of the emerging field of dance medicine and science is improved prevention, diagnosis, treatment, and rehabilitation of dance injuries.”[74]
From a psychological perspective, it is important for dancers to be understood by their practitioners, as dancers want to feel comfortable knowing that their medical personnel and teachers understand their injury, lifestyle, and the implications of the injury for their participation in dance. They do not want to be told to stop dancing, and they want the practitioner to understand that, unlike some athletes, dancers do not have an “off season.” Dancers often rehearse for large shows or a series of shows in a concentrated period, so that a two-week break from practice, which may seem negligible to the medical person, may well seem catastrophic to the dancer. Reporting and treatment of injuries, or lack thereof, is very much tied to psychological and psychosocial issues such as personal beliefs, perceived risks, available social support, and the culture of tolerance. Assessment and treatment of injuries should include a careful history and consideration of intrinsic factors, such as “associated illness, nutrition, cultural de-conditioning, and psychosocial stress.”[75]
Stress, Injury, and Social Support
A relationship has been demonstrated between increased stress and injury in sport[19,76-79] and dance.[7,13] Evidence from research on dance injury suggests that negative life stress (events such as a difficult relationship with a peer or teacher that are interpreted by the individual as negative) is related to duration of injury,[6] maladaptive sub-scales of perfectionism,[2] injury onset,[7] and the number and severity of injuries in dance.[12] Garrick and Requa found that 23% of the dancers in their study accounted for 52% of all injuries and hypothesized that there may be potential injury vulnerability factors with respect to injuries sustained.[80] They suggested a need for more research into the risk factors associated with injuries to dancers.
To answer this call, Patterson and colleagues investigated, prospectively, the relationships among stress, injury, and social support.[81] Consistent with the research showing that social support has a buffering effect on stress, their results suggested that high negative life stress and low social support may place dancers at increased risk for injury. [82-84] Their finding that negative life stressors (also defined as “microstressors” or “daily hassles”) are related to injuries only in dancers who report low levels of social support speaks to the importance of promoting supportive environments in order to buffer the impact of stress. It follows that social support is an important ingredient in the management of dance injuries. Research and related dancers’ experiences indicate that dancers often do not receive sufficient social support once injured.[13,14] Injury is a disruptive life event for most and, for some dancers, a traumatic life event. Logically, if negative life events contribute to the onset of injury (as research indicates), an injury would, in turn, compound the negative stress. Therefore, it is not surprising that dancers experience negative mood states after an injury.
Given what we know about stress, injury, and reactions to injury, it is critical that injured dancers perceive that they are getting adequate social support. Peers, dance educators, dance companies, friends, choreographers, medical personnel, and loved ones can facilitate injury recovery by supporting the injured dancer. What, then, constitutes appropriate social support for the injured dancer? Mainwaring found that a group of athletes with severe knee injuries did not appreciate certain kinds of help.[24] For example, most did not like sympathy or being viewed as “disabled,” and they especially abhorred having doors held open for them when they were on crutches. It may be that, for injured dancers, appropriate social support means helping them to rest or modify their training according to sound medical advice. Time spent with peers may also be crucial, especially when that involves events other than merely observing classes and rehearsals.
As we have acknowledged, most dancers continue to dance despite injuries, or hasten their return to rehearsal or performance to their own detriment, because they perceive that “others” expect them to continue to work through the injury. Appropriate social support and understanding is critical. It may well be the friend, the artistic director, or the practitioner who validates the emotional upheaval and the “disrupted sense of self ” that accompany injury. Giving the dancer assurance that there will not be negative judgments surrounding time off or work modifications may be an essential element of support.
Culture of Injury, Pain, and Tolerance
The dance community subscribes to a subculture that reinforces certain beliefs and values about pain, tolerance, perseverance, and accepting and ignoring injury. This systemic “culture of injury, pain, and tolerance” encourages behavior that predisposes the dancer to risk of injury (primarily overuse) and chronic pain. A similar subculture has been well documented recently in sport.[71,72,85] Nixon suggested that injuries and pain are normal in sport and that athletes are exposed to a:
set of beliefs about structural constraints, structural inducements, general cultural values and processes of institutional rationalization and athletic socialization that collectively convey the message that they ought to accept the risks, pain and injuries of sport.[72]The culture of dance, like sport, also encourages dancers to be constantly aware of their body image,[86] weight, and food intake. Hence, when injury requires a dancer to reduce or modify training, weight gain is often a concern. Dancers frequently will equate the loss of muscle tone that may accompany injury with “getting fat.” Consequently, caloric intake may be reduced to dangerous levels.[87] The relationship between eating disorders and injury onset has been established, [88-90] but disordered eating as a consequence of injury has not yet been investigated.
Implications for Research, Teaching, and Clinical Practice
It is evident from this review that the psychological impact of physical injury on dancers is not well understood, and is only just beginning to be addressed in current research. This has broad implications for the dancer, the educator, the clinician, and the scientist. First, we need to understand the reaction to injury from a dancer’s perspective. There are issues unique to dancers that may influence psychological reactions,[91] and thus physical recovery.
Directions for research are multifaceted and include the identification of the following:
• Subjective experiences of dance injury;
• Personality correlates of stress and injury;
• Psychophysiological markers of stress throughout the injury process;
• Coping styles and strategies;
• Moderator variables for pain experiences in dance (e.g., the meaning of pain to the individual);
• Differences in emotional reactions to acute and overuse injuries;
• Appropriate and accepted forms of social support following dance injury;
• Systemic factors that contribute to a subculture of injury, pain, and tolerance;
• Issues of eating behaviors after injury; and
• Education and intervention strategies for psychological management of dance injuries.
These are exciting opportunities for research.
From an educational perspective, recommendations and materials from research, experience, and clinical expertise should be developed to help the dancer manage the psychological reaction to injury. For example, Mainwaring and Krasnow suggested a variety of approaches for the dance teacher or choreographer dealing with an injured dancer, including educating and assisting the dancer to better understand how to modify dance activities during the rehabilitation period in a manner that still allows for improvement, and continuing verbal support and correction.[14] Giving the dancer more say about the use of a temporary understudy replacement, thereby reducing the fear that his or her part will be permanently lost, may be important. If the dancer is totally unable to participate, the teacher can ask her or him to assist in classes, coach other students outside class time, and assist in rehearsals (taking and giving notes, coaching other dancers who are struggling with sections of the work, and similar roles). Reactions to watching class vary in each individual, and the teacher should allow the dancer to use class time for activities such as physiotherapy or personal work if she or he is one who finds passive observation depressing and frustrating rather than useful. Further suggestions include giving the dancer readings and film/ video viewing to sustain interest and motivation, encouraging imagery work, engaging in discussions with medical personnel and family (making sure to include the dancer in these exchanges), and establishing realistic goals with the dancer, in concert with the medical personnel.
Clinical management of injuries could be facilitated with a greater appreciation of the psychological sequelae of injury. For example, dancers want to feel that their practitioner understands that refraining from dance is not the best option for them and their lifestyle. The dancer-practitioner relationship is an important element in adherence to rehabilitation; an understanding of the psychological context of injury can facilitate that relationship. The following excerpt from Ryan and Stephen’s book promotes the whole person and multidisciplinary approach to rehabilitation that incorporates many of the psychological concepts considered in this paper:
Whether an illness or injury has caused a dancer to stop dancing entirely for a short or long time or has simply forced him or her to reduce the workload, his or her mind should be set on getting back to normal activity as soon as possible. Rehabilitation describes that process in brief, but doesn’t specify what it means in terms of objectives, methods and goals and the persons who must necessarily be involved.Each step should be in a logical progression so that it builds on the preceding steps to move smoothly towards the stated goal. If surgical treatment is part of the program physical therapy may be appropriate before as well as after surgery. Psychological counseling for adapting to the particular surgery should begin before the surgery. Improvement of nutritional practices, if necessary, should not have to wait until the treatment…has finished.[68]
Contemporary research on dance injuries is helping to address longstanding psychological issues and to improve the multidisciplinary management of dance injuries. For example, the book by Solomon and colleagues expresses the importance of both the “psyche” and the body in preventing dance injuries.8 The book’s dedication is poignant: “To Jean Erdman, who taught me to teach so that the individual artist in each of us could emerge without damage to the body or psyche. R.S.”8 Appreciating the impact and sequelae of dance injuries from a psychological perspective not only provides us with information about recovery, but also points to issues (such as being understood by practitioners, the reporting of injuries, and sound teaching practices) that can be addressed and may facilitate injury prevention.
In general, the information reviewed here emphasizes that dance medicine, dance science, and dance psychology are contributing to a pool of knowledge regarding injury prevention and management which endorses the view that…
Acknowledgment
The authors would like to thank Enid K. Headley, Christine Provvidenza, Jennifer Jones, and the editors for their comments and suggestions for earlier drafts of the paper and the model.
REFERENCES
1. Caine C, Garrick J: Dance. In: Caine D, Caine C, Lindner K (eds): Epidemiology of Sports Injuries. Champaign, IL: Human Kinetics, 1996, pp.124-160.
2. Krasnow D, Mainwaring L, Kerr G: Injury, stress, and perfectionism in young dancers and gymnasts. J Dance Med Sci 3(2):51-58,1999.
3. Lewis R, Dickerson J, Davies G: Lifestyle and injuries of professional ballet dancers: reflections in retirement. J Royal Society of Health 117(1):23-31, 1997.
4. Macchi R, Crossman J: After the fall: Reflections of injured classical ballet dancers. J Sport Behav 19(3):221-234, 1996.
5. Macintyre J, Joy E: Foot and ankle injuries in dance. Clinics in Sport Med 2:351-368, 2000.
6. Krasnow D, Kerr G, Mainwaring L: Psychology of dealing with the injured dancer. Med Probl of Perform Art 9:7-9, 1994.
7. Liederbach M, Gleim G, Nicholas, J: Physiologic and psychological measurements of performance stress and onset of injuries in professional ballet dancers. Med Probl of Perform Art 9:10-14, 1994.
8. Solomon R, Minton S, Solomon J: Preventing Dance Injuries: An Interdisciplinary Perspective. Reston, VA: American Alliance for Physical Education, Recreation and Dance, 1990.
9. Solomon, R, Micheli, LJ: Concepts in the prevention of dance injuries: A survey and analysis. In: Shell, CG (ed), The Dancer as Athlete: The 1984 Olympic Scientific Congress Proceedings, 8. Champaign, IL: Human Kinetics Publishers, Inc., 1986 pp. 201-212, 1986.
10. Solomon, R, Micheli, LJ: Technique as a consideration in treating modern dance injuries. Physician and Sportsmedicine 14(8):83-92, Aug. 1986.
11. Pedersen M, Wilmerding V: Injury profiles of student and professional flamenco dancers. J Dance Med Sci 3:108-114, 1998.
12. Hamilton LH, Hamilton WG, Meltzer JD, Marshall P, Molnar M: Personality, stress, and injuries in professional ballet dancers. Am J Sports Med 17:263-267, 1989.
13. Mainwaring L, Kerr G, Krasnow D: Psychological correlates of dance injuries. Med Probl Perform Art 8:3-6, 1993.
14. Mainwaring L, Krasnow D: Psychological response to hip injuries in the young elite dancer. Presented at the International Association for Dance Medicine and Science Conference, Tring, England, October 1999.
15. Hamilton L: A psychological approach to the rehabilitation of injured performers. Orthopaedic Physical Therapy Clinics of North America 6(2):131-143, 1997.
16. Hamilton L, Hamilton W, Warren M: Injury prevention in ballet: Physical, nutritional and psychological considerations. Presented at the Annual APA Convention, Toronto, 1993.
17. Gordon S: Sport psychology and the injured athlete: A cognitive-behavioural approach to injury response and injury rehabilitation. Science Periodical on Research and Technology in Sport, pp.1-10, 1986.
18. Mainwaring L, Galway R: Psychological factors of athletic injury rehabilitation. In: Giam CK, Chook KK, The KC (eds): Conference Proceedings for the 7th World Congress of the International Society for Sport Psychology. Singapore, 1989.
19. May J, Sieb G. Athletic injuries: Psychosocial factors in the onset, sequelae, rehabilitation and prevention. In: May JR, Asken MJ (eds): Sport Psychology: The Psychological Health of the Athlete. New York: PMA Publishing, 1987, pp.157-185.
20. Pedersen P: The grief response and injury: A special challenge for athletes and athletic trainers. Athletic Training 21(4):312-314, 1986.
21. Rotella RJ, Heyman SR: Stress, injury, and the psychological rehabilitation of athletes. In: Williams J (ed): Applied Sport Psychology: Personal Growth to Peak Performance. Palo Alto CA: Mayfield, 1986, pp.343-364.
22. Andersen M, Williams J: A model of stress and athletic injury: Prediction and prevention. J Sport Exer Psych 10:294-306, 1988.
23. Brewer BW: Review and critique of models of psychological adjustment to athletic injury. J Appl Sport Psych 6:87-100, 1994.
24. Mainwaring L: Restoration of self: A model for the psychological response of athletes to severe knee injuries. Canadian Journal of Rehabilitation 12(3):145-156,1999.
25. Rose J, Jevne R: Psychosocial processes associated with athletic injuries. Sport Psych 7:309-328, 1993.
26. Wiese-Bjornstal DM, Smith AM, Schaffer SM, Morrey MA: An integrated model of response to sport injury: Psychological and sociological dynamics. J Appl Sport Psych 10(1):46-69, 1998.
27. Eaton D: A study of the emotional responses and coping strategies of male and female athletes with moderate and severe injuries. Unpublished Doctoral Dissertation, Western Michigan University, 1996.
28. Heil J: Psychology of Sport Injury. Champaign, IL: Human Kinetics, 1993.
29. Granito V, Carroll, J: Psychological response to athletic injury: Themes from intercollegiate athletes. Presented at the Association for the Advancement of Applied Sport Psychology Conference, Nashville, TN, 2000.
30. Leddy MH, Lamber MJ, Ogles BM: Psychological consequences of athletic injury among high-level competitors. Res Quart Exer Sport 65(4):347-354, 1994.
31. Smith A, Scott S, O’Fallon M, Young M: Emotional responses of athletes to injury. Mayo Clinic Proceedings 65: 38-50, 1990.
32. Williams JM, Roepke N: Psychology of injury and injury rehabilitation. In: Singer RN, Murphey M, Tennant LK (eds): Handbook of Research on Sport Psychology. New York: MacMillian, 1993, pp. 815-39.
33. Brewer BW: Self-identity and specific vulnerability to depressed mood. Journal of Personality 61:343-364, 1993.
34. May J. Veach T, Reed M, Griffey M: A psychosocial study of health injury and performance in athletes on the U.S. Alpine ski team. Phys Sportsmed 13:111-115, 1985.
35. Quackenbush N, Crossman J: Injured athletes: A study of emotional responses. J Sport Behav 17:178-187, 1992.
36. McDonald S, Hardy J: Affective response patterns of the injured athlete: An exploratory analysis. Sport Psych 4:261-274, 1990.
37. LaMott, EE: The anterior cruciate ligament injured athlete: the psychological process. Unpublished Doctoral Dissertation, University of Minnesota, 1994.
38. Johnson U: The multiply injured versus the first-time-injured athlete during rehabilitation: A comparison of nonphysical characteristics. J Sport Rehab 5:293-304, 1996.
39. Wasley D, Lox CL: Self-esteem and coping responses of athletes with acute versus chronic injuries. Perceptual and Motor Skills 86:1402, 1998.
40. Smith A: Psychological impact of injuries in athletes. Sports Med 22(6):391-405, 1996.
41. Pearson L, Jones G: Emotional effects of sports injuries: Implications for physiotherapists. Physiotherapy 78:762-770, 1992.
42. Suinn RM: Psychological reactions to physical disability. Journal of the Association for Physical and Mental Rehabilitation 21(1):13-15, 1967.
43. Gordon S, Milios K, Grove R.J: Psychological aspects of the recovery process from sport injury: The perspective of sport physiotherapists. The Australian Journal of Science and Medicine in Sport 23(2):53-60, 1991.
44. Flint FA: The psychological effects of modeling in athletic injury rehabilitation. Doctoral Dissertation, University of Oregon, 1991.
45. Grove JR, Stewart RML, Gordon S: Emotional reactions of athletes to knee rehabilitation. Presented at the annual meeting of the Australian Sports Medicine Federation, Alice Springs, Australia, 1990.
46. Ford IW, Gordon, S: Perspectives of sport trainers and athletic therapists on the psychological content of their practice and training. J Sport Rehab 7:79-94, 1988.
47. Ahern D, Lohr B: Psychosocial factors in sports injury rehabilitation. Clin Sport Med 16(4):755-768, 1997.
48. Williams J, Rotella R, Heyman S: Stress, injury, and the psychological rehabilitation of athletes. In: Williams J (ed): Applied Sport Psychology: Personal Growth to Peak Performance. Palo Alto, CA: Mayfield Publishing Company, 1986, pp.409-428.
49. Wiese-Bjornstal K, Smith A: Counseling strategies for enhanced recovery of injured athletes within a team approach. In: D. Pargaman (ed): Psychological Bases of Sport Injuries. Morgantown, WV: Fitness Information Technology, 1993, pp.149-182.
50. Williams J, Roepke N: Psychology of injury and injury rehabilitation. In: Singer R, Murphey M, Tenant LK (eds): Handbook of Research on Sport Psychology. New York: Mac Milan, 1993, pp. 815-839.
51. Lundon K, Melcher L, Bray K: Stress fractures in ballet: A twenty-five year review. J Dance Med Sci 3:101-107, 1999.
52. Pedersen E, Wilmerding V: Injury profiles of student and professional flamenco dancers. J Dance Med Sci 2(3):108-114, 1998.
53. Bowling A: Injuries to dancers: Prevalence, treatment, and perceptions of causes. BMJ 298:731-734, 1989.
54. Kerr G, Krasnow D, Mainwaring L: The nature of dance injuries. Med Probl Perform Art 7:25-29, 1992.
55. Schafle M, Requa R, Garrick J: A comparison of patterns of injury in ballet, modern, and aerobic dance. In: Solomon R, Minton S, Solomon J (eds): Preventing Dance Injuries: An Interdisciplinary Perspective. Reston, VA: American Alliance for Health, Physical Education, Recreation and Dance, 1990, pp.1-14.
56. Liederbach M: General considerations for guiding dance injury rehabilitation. J Dance Med Sci 4(2):54-65, 2000.
57. Tajet-Foxell B. Rose F: Pain and pain tolerance in professional ballet dancers. British J Sport Med 29(1):31-34, 1995.
58. Melzack R: The short form McGill Pain Questionnaire. Pain 30:191-197, 1987.
59. Ramel E, Moritz U, Jarnlo G: Recurrent musculoskeletal pain in professional ballet dancers in Sweden: A six-year follow-up. J Dance Med Sci 3:93-100, 1999.
60. Encarnacion M, Meyers M, Ryan N, Pease D: Pain coping styles of ballet performers. J Sport Behav 23(1):20-32, 2000.
61. Meyers MC, Bourgeois AE: Predicting pain response in athletes: Development and assessment of the Sports Inventory for Pain. J Sport Exer Psych 14:249-261, 1992.
62. Checkley S: The neuroendocrinology of depression and chronic stress. British Medical Bulletin 52(3): 597-617, 1996.
63. Rietveld B: Dance injuries in the older dancer: Comparison with younger dancers. J Dance Med Sci 4(1):16-19, 2000.
64. Carver CS, Pozo-Kaderman C, Harris SD, et al: Optimism versus pessimism predicts the quality of women's adjustment to early stage breast cancer. Cancer 73:1213-1220, 1994.
65. Fischer CA, Domm MA, Wuest DA: Adherence to sports-related rehabilitation programs. Phys Sportsmed 16:47-52, 1988.
66. Scheier MF, Carver CS: Optimism, coping, and health: Assessment and implications of generalized outcome expectancies. Health Psych 4:219-247, 1985.
67. Scheier MF, Carver CS: Dispositional optimism and physical well-being: The influence of generalized outcome expectancies on health. J Pers 55:169-210, 1987.
68. Ryan AJ, Stephens, RE: Rehabilitation from dance injuries. In: Ryan AJ, Stephens, RE (eds): The Dancer’s Complete Guide to Healthcare and a Long Career. Chicago, IL: Bonus Books. 1988, pp. 160-164.
69. Charmaz K: Identity dilemmas of chronically ill men. Soc Quart 35(2):269-288, 1994.
70. Charmaz K: The body, identity, and self: Adapting to impairment. Soc Quart 36(4):657-680, 1995.
71. Sparkes A: Athletic injury: An Achilles' heel to the survival of self. Qualitative Health Research 8(5):644-664, 1998.
72. Nixon H: Accepting the risks of pain and injury in sport: Mediated cultural influences on playing hurt. Sociology of Sport Journal 10:183-196, 1993.
73. Shaffer, SM: Attributions and self-efficacy as predictors of rehabilitative success. Master's Thesis, University of Illinois, 1992.
74. Trepman E: The treatment and rehabilitation of dance injuries. J Dance Med Sci 4(1):5, 2000.
75. Luke A, Micheli LJ: Management of injuries in the young dancer. J Dance Med Sci 4(1):6-15, 2000.
76. Bramwell S, Masuda M, Wagner V, Homes T: Psychosocial factors in athletic injuries. J Hum Stress 1:6-20, 1975.
77. Cryan P, Alles W: The relationship between stress and college football injuries. J Sports Med 23: 52-58, 1983.
78. Passer, M, Seese M: Life stress and athletic injuries: Examination of positive versus negative events and three moderator variables. J Hum Stress 9: 11-16, 1983.
79. Smith R, Smoll F, Ptacek J: Conjunctive moderator variables in vulnerability and resiliency research: Life stress, social support and coping skills, and adolescent sport injuries. J Pers Soc Psych 58(2): 360-370, 1990.
80. Garrick J, Requa R: Ballet injuries: An analysis of epidemiology and financial outcome. Am J of Sports Med 21:586-590, 1993.
81. Patterson E, Smith R. Everett J, Ptacek J: Psychosocial factors as predictors of ballet injuries: Interactive effects of life stress and social support. J of Sport Behav 21(1):101-111, 1998.
82. Cohen S, Syme SL: Social Support and Health. New York: Academic Press, 1985.
83. Petrie TA: Psychosocial antecedents of athletic injury: the effects of life stress and social support on female collegiate gymnasts. Behav Med 18:127-138, 1992.
84. Sarason IG, Sarason BR, Pierce GR (eds): Social Support: An Interactional View. New York: Wiley, 1990.
85. Kotarba JA: Chronic Pain: Its Social Dimensions. Beverly Hills, CA: Sage, 1983.
86. Pierce E, Daleng M: Distortion of body image among elite female dancers. Percep Motor Skills 87:769-770, 1998.
87. Culnane C, Deutsch D: Dancer disordered eating: Comparison of disordered eating behaviour and nutritional status among female dancers. J Dance Med Sci 2(3):95-100,1998.
88. Hamilton L, Brooks-Gunn J, Warren M, Hamilton W: The impact of thinness and dieting on the professional dancer. CAPHER J 52(4):30-35, 1986.
89. Micheli LJ, Solomon R: Stress fractures in dancers. In: Solomon R, Minton SC, Solomon J (eds): Preventing Dance Injuries: An Interdisciplinary Perspective. Reston, VA: American Alliance for Health, Physical Education, Recreation and Dance, 1990, pp.133-153.
90. Kaufman B, Warren M, Hamilton L: Intervention in an elite ballet school: An attempt at decreasing eating disorders and injury. Women's Studies International Forum 19(5):545-549, 1996.
91. Hamilton L, Kella J, Hamilton W: Personality and occupational stress in elite performers. Med Probl Perform Art 10:86-89, 1995.
92. Taylor J, Taylor C: Psychology of Dance. Champaign, IL: Human Kinetics, 1995.